Published: June 16, 2024 | 8 mins read
Cystine Kidney Stones: Subtypes and Causes
ARTICLE SHORTCUTS
Cystine stones are somehow the black sheep in the kidney stone family. It is the only stone type that is totally brought by bad genes. Luckily, only about 1% to 2% of stone-formers have to deal with these misfits.
But the sad thing is that people who have cystine stones often form kidney stones every one to two years. And the really bonkers part? These stones have an 83% recurrence rate within five years—higher than any other type!
If you’re a cystine stone-former, you’re probably thinking right now, “I’m doomed!”
Wait, don’t give up all hope just yet. It’s not totally clobbered. There’s a way out of the hole, which we will dig into later.
But first, let’s familiarize ourselves with our goofy subject – cystine stones.
Background
Again, cystine stones are like your wacky brother, fraying you to your nerve, thanks to some lousy genes.
For more accurate figures, cystine stones account for 1% of adult and 6%- 8% of childhood kidney stones in the United States. All thanks to a genetic prankster called cystinuria. Cystinuria happens when there’s an inherited defect in the transport of the amino acid cystine. This leads to more cystine in the urine, which can crystallize under specific conditions. We have a separate blog on cystinuria; check it out here to get more details.
Anyway, cystinuria only pops up in about 1 in 10,000 people, adding up to around 33,000 new cases every year. Globally, it’s about 1 in 7,000 people, but the numbers vary depending on where you are.
While the overall risk of some kind of kidney injury or failure is high, up to 70%, the chance of reaching end-stage renal failure is relatively low, thankfully under 5%.
But, the unfortunate truth is that the average onset age for cystine stones is around 22 years, and around 22% of cystinuria patients develop stones during childhood. That means by the time you are supposed to enjoy your youth, you are instead suffering from kidney stones.
If you are a cystine stone-former, you’ll likely recognize either of the two subtypes we will discuss in the next chapter.
Cystine Stone Subtypes
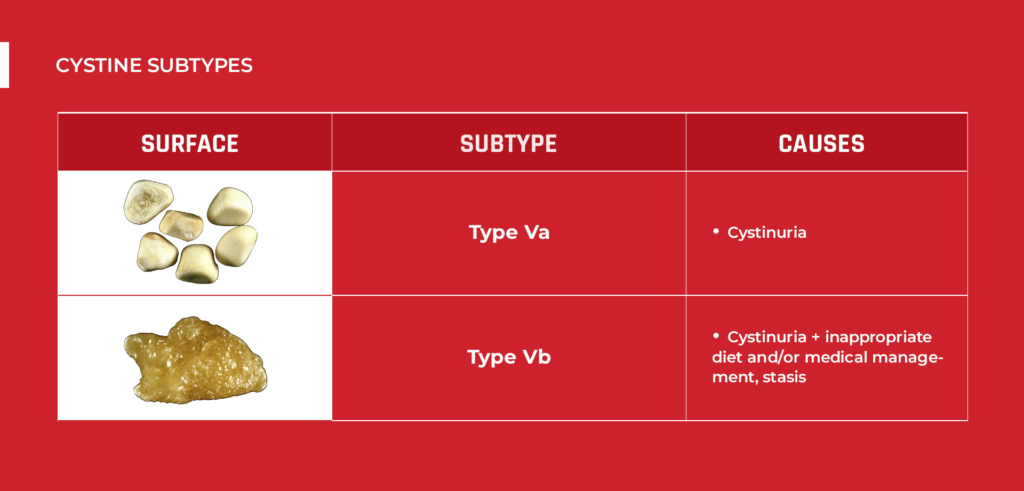
Cystine stones have two subtypes. Though both of them are brought by cystinuria, there are still unique differences worth noting.
TYPE Va
This subtype is the most common one. In fact, type Va is about ten times more frequent than type Vb stones. Here are its characteristics:
- Rough surface
- Yellowish color
Internally, type Va stones are yellowish, poorly organized, and sometimes have a radiating organization. Cystinuria is the primary reason why they form. Type Va stones are dense because they are purely cystine. Most cystine stone patients have a stone density ranging from around 400 to 800 HU (Hounsfiled Units). However, in rare cases, type Va stones can reach a density of around 1000 HU.

TYPE Vb
Type Vb stones are less frequent than Type V stones. Here are its characteristics:
- Smooth surface
- Homogeneous (even)
- Cream to yellowish in color
Type Vb stones usually form in numbers, which could be the secret behind their smooth surface. The stones are likely rubbing against each other as they are confined in the kidney.
Internally, you will notice concentric layers at the periphery and an unorganized core. The periphery has a cream hue, while the core is yellowish.
Unlike type Va stones, type Vb is caused not only by cystinuria but also by inappropriate diet and/or medical management and urinary stasis (urine not draining completely).
Since these stones are less compact than type Va stones, they tend to be very weak, only around 109 to 192 HU. Okay, now that you’re familiar with the two cystine stone subtypes, let’s explain how cystinuria leads to kidney stone formation.

Cystine Stone Causes
When there’s too much cystine partying in your urine, it can lead to stone formation. In people without cystinuria, the daily amount of cystine in urine is typically less than 30 mg. However, in those with cystinuria, it can be over 300 mg per day. In children, doctors sometimes use a spot urine test called cystine/creatinine ratio to check for cystinuria:
- Less than 80 mg/g creatinine for infants under 1 month
- Less than 52 mg/g creatinine for infants between 1-12 months
- Less than 35 mg/g creatinine for those over 1 year
But here’s a secret: cystinuria wouldn’t be a problem if your urine’s pH is around 7.0 to 7.5. At a pH of 7.0, the amount of cystine that can dissolve in urine is around 250 mg/L. This increases as the urine becomes more alkaline. For example, at a pH of 7.5, about 500 mg of cystine can dissolve in a liter of urine. Be careful, though; if your urine pH goes over 7.5, you might be setting up the stage for another stone type, calcium phosphate stones. So, think about it like balancing on a scale. You can’t go further on either side.
Anyway, around 20% to 40% of people with cystine stones also have other kidney stone risk factors, such as low citrate levels (found in 44% of cases). This is why about a quarter of people with cystinuria can develop non-cystine kidney stones as well.
Oh! We almost forgot. Let’s talk about the mechanism of how cystinuria causes all this trouble. The section below will give you an idea.
The Mechanism Behind Stone Formation
When you have cystinuria, the transporters responsible for reabsorbing cystine in the kidney tubules become defective. As a result, a lot of cystine remains in urine instead of being reabsorbed back into the bloodstream. Excess amounts can become too much for the urine to hold.
In time, these cystine molecules come in contact with each other and form crystal aggregates. The strong and stable disulfide bonds (made of two sulfur atoms) between cystine molecules hold these aggregates together, allowing them to grow and form larger structures, eventually leading to cystine kidney stone formation.
So, while cystine is the primary component of cystine stones, the disulfide bonds formed within cystine molecules play a crucial role in holding the stones together and contributing to their durability.
After learning all this information about cystine stones, how do you translate this knowledge into treatment/prevention? The next chapter is the ultimate gold mine.
Treatment and Prevention Strategy
As mentioned earlier, there are two types of cystine stones – type Va and Vb.
Since type Va stones are dense, they may not break apart using CLEANSE if their density is over 750 HU. But worry not—stones up to 9 mm in diameter (not just length or width) can pass with CLEANSE.
Meanwhile, type Vb stones are very weak and can easily dissolve with natural supplements, like CLEANSE.
So, while cystine stones are genetic and almost a lifetime burden for those who have them, there’s always a light at the end of this stony tunnel.
Also, prevention is possible naturally. Most doctors advise taking thiol-based drugs, as they help break disulfide bonds. However, taking drugs isn’t always the best solution. The real deal is urine pH. Remember, cystine stones don’t form at a pH of 7.0 to 7.5. So, the goal is to keep your urine pH at that range only. Using pH test strips at home to test your urine pH regularly would be great.
At this point, doctors would usually advise, “Hey, eat less meat and munch on more plants.” – WRONG.
Most doctors give this misleading advice simply because cystine is an amino acid abundant in meat. However, cystine is an essential amino acid. It’s not the enemy. The problem is on the transport of cystine, not cystine itself.
Also, eating plant-based diets is unsuitable as the goal isn’t to over-alkalize your urine but to keep it neutral. You can achieve that through an animal-based diet. Why? Because the real reason why urine becomes acidic isn’t meat or salt but metabolic issues (being overweight, etc.). Going animal-based is the key to cleaning up your diet and becoming metabolically healthy. If you eat plant-based diets, you’ll put yourself at risk of calcium oxalate or calcium phosphate stones.
If you want help in cleaning up your diet to make sure you are not putting yourself at risk of cystine kidney stones, we invite you to our Coaching Program. This is your chance to break free from the false narrative that bad genes automatically mean “game over.” The wheels are yours to maneuver.
REFERENCE:
- Clinical utility of computed tomography Hounsfield characterization for percutaneous nephrolithotomy: a cross-sectional study
- Comprehensive morpho-constitutional analysis of urinary stones improves etiological diagnosis and therapeutic strategy of nephrolithiasis
- Cystinuria: An Overview of Challenges and Surgical Management
- Cystinuria: An Overview of Diagnosis and Medical Management
- Efficacy of Hounsfield Unit of CT in Prediction of the Chemical Composition of Urinary Stones
- Hounsfield Measurements for Detection of Stone Composition, Density, and Overall Hardness – A Brief Report
- International Cystinuria Foundation
- The comparative survey of Hounsfield units of stone composition in urolithiasis patients
- Usefulness of hounsfield unit and density in the assessment and treatment of urinary stones

Fact Checked by Joey Weichmann
Written by
The Stone Relief Team
Joey Weichmann (aka “The Stone Slayer”) is the Founder of Stone Relief. As an avid naturopath and kidney stone sufferer, Joey has made it his mission to help health-conscious individuals stop kidney stones and get their life back.
Comments or questions?
Responses
WHAT TO READ NEXT
Publish Date: August 18, 2024
Staghorn Kidney Stones Are BIG Problems!
Publish Date: August 4, 2024
Brushite Stones: The Most Complex Kidney Stones
Publish Date: July 28, 2024
The Deadly Struvite Stones