Published: January 10, 2022 | 1 min read
Kidney Stone Imaging Techniques [What Should You Choose?]
ARTICLE SHORTCUTS
The imaging you receive for your kidney stone can either set you up for success or leave you hanging without critical information. This blog aims to equip you with the knowledge you need to have an educated conversation with your Doctor/Urologist to ensure you receive the appropriate imaging technique for your specific situation.
BACKGROUND
Before we start evaluating the different imaging techniques in current use, let’s set the foundation for comparison. First, we will assess the different imaging techniques based on their sensitivity and specificity:
- Sensitivity: Probability of a positive diagnostic test in a patient with the illness or injury.
- Specificity: Probability of a negative diagnostic test in a patient free of the disease or injury.
The higher the sensitivity and specificity, the better chance of identifying a kidney stone.
Next, we will be evaluating the type of imaging available. Traditional 2D imagery can help identify a stone location and rough approximation of size. However, 3D imaging can provide a level of detail that far surpasses 2D. While 3D imaging provides more information, it may not always be necessary information, depending on where you are at in your kidney stone journey.
Radiation exposure is the following criteria for evaluation. When it comes to imaging, radiation provides a much more powerful analysis and ability to spot kidney stones. However, this comes at a cost to our bodies as radiation accumulates over our lifetime. Malignancy issues have been observed in as little as 100 mSv (mSv= Millisiviert= unit measuring radiation doses).
The ability to identify Hydronephrosis is another instrumental piece of information that can be obtained from imaging. Hydronephrosis is swelling of the kidneys when urine can’t drain. Mild stages of Hydronephrosis are standard when you have a kidney stone. But, it can become severe and is very important for Doctors and Urologists to identify at the time of imaging to prescribe appropriate treatment.
Lastly, we will compare the average cost of each procedure. Having a kidney stone can be an expensive proposition, sometimes in the neighborhood of $10,000+ per occurrence with decent insurance. So, weighing out the cost benefits of each technique becomes an important consideration.
CT SCAN

In the United States, Computerized Topography (CT Scan- a.k.a. “Cat Scan”) is the gold standard of care for kidney stones. CT scans work by exploiting the different degrees to which our body tissues absorb radiation. Multiple data points are obtained during a scan by rotating a radiation source with a detector on the opposite side around the patient. A computer then processes these data points into a 3D image, thus “computerized” topography or “CT Scan.”
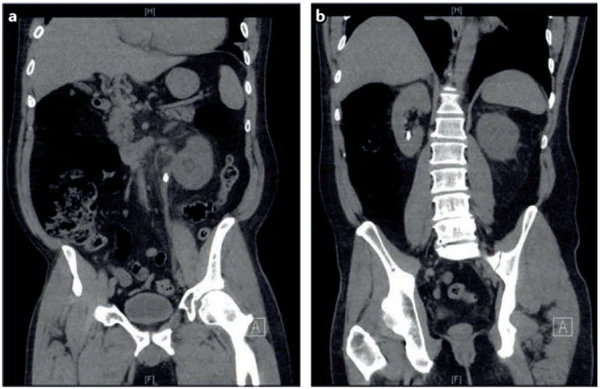
Kidney stones have a markedly different composition when compared to the rest of the urinary tract and absorb considerably more radiation (see image below). This makes kidney stones easily identifiable without the need for contrast (dye used to contrast different parts of the body). Due to the ease of spotting kidney stones with a CT scan, the sensitivity is rated at 95% and specificity at 98%.
This high percentage performance makes the CT scan the first-line choice for most Doctors and Urologists in the United States. However, CT scans can suffer identification issues with stones smaller than 3mm as stones of this size may slip between the imaged tissue planes and not be detected.
An added benefit of using CT scans is their ability to provide information regarding the composition of stones. Attenuation describes the density of objects encountered by photons passing from the radiation source to the detector. The Hounsfield Unit is a measurement of attenuation. On this scale, water is given a value of 0 HU, air is -1,000 HU, and bone is 1,000 HU. The Hounsfield Unit of a stone can indicate its type, as different stone compositions absorb differing amounts of radiation.
Understanding the density of kidney stone types is incredibly beneficial. Not only can different therapy decisions be made on how to best manage the passing of the kidney stone without surgery, but decisions regarding responsiveness to shock-wave lithotripsy can also be made if a surgical intervention is deemed necessary.
While CT scans are incredibly powerful for identifying kidney stones, they do come at a cost. And that cost is paid in terms of radiation exposure. A traditional non-contrast CT scan will expose you to ~10 mSv, while a low-dose CT scan will expose you to < 3 mSv. An ultra-low dose CT scan option is available with exposure at less than 1 mSv. But, with a decrease in radiation, comes a decrease in sensitivity and specificity which ultimately impacts the ability to identify kidney stones. If you are obese (BMI > 30), a low-dose CT scan will not be an option.
And, speaking of costs, CT scans are one of the most expensive imaging techniques. The average cost for a non-contrast CT scan in the United States is $1,000.

ULTRASOUND

Ultrasonography is a low-cost imaging technique that does not utilize ionizing radiation like CT scans or X-Rays. Outside of the United States, Ultrasound is becoming the primary first-line imaging technique and is the current standard for young and pregnant patients. While CT scans are the primary first-line tool in the United States, Ultrasound is gaining popularity.
Imagery obtained from an ultrasound is produced when a transducer delivers short bursts of acoustic energy to the patient. This acoustic energy propagates through tissues in the body as waves. These waves are partially reflected back to the source (transducer) when passing between tissues of different densities and/or acoustic impedances (how easy a sound wave moves through different mediums/tissues). A receiver then detects the reflected waves allowing for 2D images to be generated based on wave travel times and amplitude.
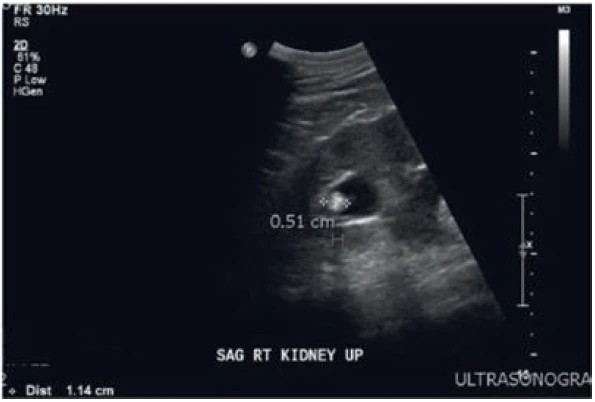
Like with a CT scan, Ultrasonography makes use of physical differences between kidney stones and surrounding tissues to detect the stones. Relative to soft tissues, kidney stones strongly reflect ultrasonic waves and appear as bright echoic structures in the ultrasonographic image (see image below). Since ultrasonic waves cannot penetrate kidney stones, a non-echogenic (meaning that it cannot return the signal from an ultrasound machine) shadow is visible beyond the kidney stone in the image. Ultrasounds can also detect Hydronephrosis.
A wide range of sensitivities and specificities for Ultrasonography has been reported. A pooled review of the literature demonstrates a sensitivity of 45% and specificity of 88% for kidney stones. Sensitivity is reduced for stones < 3mm, which might not produce a shadow. Stones can also be missed due to the difficulty of distinguishing echogenic stones from echogenic central sinus fat in the kidney.
Another limitation of Ultrasonography surrounds the estimation of stone size. The width of an ultrasound beam (and, therefore, resolution) is similar to the size of some small kidney stones. This design characteristic may result in an overestimation of actual stone size. For example, up to 50% of kidney stones < 5mm in size were measured as > 5mm in one study.
To overcome this, certain technicians will measure the shadow behind the stone, effectively measuring where the waves are absent, rather than the waves variably bounding off the front surface of the stone. Measuring stone shadow improves stone size accuracy.

In summary, Ultrasonography is currently less sensitive and specific than CT scan imagery for detecting and sizing kidney stones. However, ultrasounds have good diagnostic ability and can reliably detect the presence of Hydronephrosis. As such, this technique is recommended as the imaging technique of choice for recurrent stone formers and the first-line modality for pediatric (< 14 years old) and pregnant patients.
X-RAY

X-rays are probably the most well-known type of imaging. It is also referred to as KUB (kidney, ureter, & Bladder) plain film radiography in the kidney stone world. This imaging technique uses a single energy source to produce photons that pass through tissues in a front-to-back orientation with a receiver on the opposite end. The technique uses the same fundamental concept as a CT scan but in a single 2D plane (versus multiple planes of a 3D CT scan image).

The sensitivity and specificity of current X-ray technology is estimated at 57% and 76%, respectively. Advantages of the X-ray modality include relatively low ionizing radiation exposure (0.15 mSv) when compared to a CT scan (10 mSv) and low cost ($275 average in the United States).
X-Rays can visualize many kidney stone types. However, Cystine and Struvite stones are poorly visible, and Uric Acid sones are not visible. To compensate for this limitation, Ultrasound and X-ray techniques are often performed in conjunction, enabling higher sensitivity of ultrasound to augment the higher specificity of X-ray.

Overall, the X-ray technique is most helpful in evaluating a patient with known kidney stone disease.
MRI

Magnetic Resonance Imaging (MRI) functions by using a magnetic field to align a patients free water protons along a magnetic field axis. A radio frequency antenna is placed over the area to be imaged and releases pulses of energy that disrupt the alignment of protons. When the pulses stop, protons release energy as they realign with the magnetic field. This released energy can then be captured as an image.

The sensitivity of MRI for kidney stone imaging is variable. And, like Ultrasonography, it can be augmented by Hydronephrosis. Kidney stones can appear as a non-specific signal void using standard MRI sequences. The sensitivity of MRI, at 82%, is higher than that of an Ultrasound and X-Ray. But less than that of a CT scan.
Hydronephrosis is easily visible. However, kidney stones might not clearly be the cause of the obstruction. More often than not, a CT scan is required to detect a kidneys stone located in the ureter. When kidney stones are visualized on MRI, the modality is diagnostic, making specificity high at 98%.

A major advantage of MRI is providing 3D imaging without radiation. Unfortunately, the drawbacks of MRI prevent it from widespread use in kidney stone imaging. In general, MRI costs about three times more than a CT scan ($2,500 average cost) and has lower accuracy and much longer image acquisition times. Therefore, an MRI is most appropriately used supplementarily to an Ultrasound in pregnant patients.
SUMMARY
We just covered a lot of technical information, and we’re confident that your eyes and mind are glazed over. So, let’s simplify this as best we can:
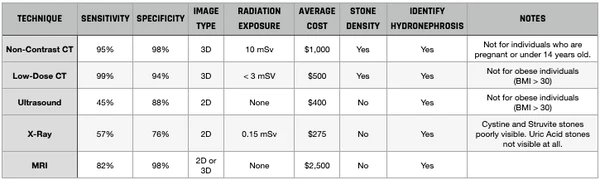
Given the information displayed in the above table, here’s how we would proceed:
- First Kidney Stone: Request a low-dose, non-contrast CT scan to be performed with your first kidney stone. You’ll pay more for this (not only in dollars but also in radiation exposure). However, the information obtained is priceless. Unlike other imaging techniques available, you will get true stone dimensions (length x width x diameter) and stone density information. Stone density, in particular, is worth its weight in gold. Certain stone types can be attacked while passing with a product like CLEANSE to break them apart to pass as gravel or sand instead of the entire stone. This stone density information can then be carried forward with future kidney stones as the type of kidney stone you form rarely, if ever, changes.
- Subsequent Kidney Stones: When it comes to your future kidney stones (and there will be more), we recommend opting for an Ultrasound. Since you already understand your kidney stone type and density from your initial CT scan, you will already know what you’re up against; as kidney stone types rarely change over time. So, obtaining a rough estimate of size, location, and hydronephrosis status with subsequent stones will more than suffice. Plus, this will be less expensive in terms of dollars and won’t cost you anything in terms of cumulative radiation exposure, as Ultrasounds do not use radiation.
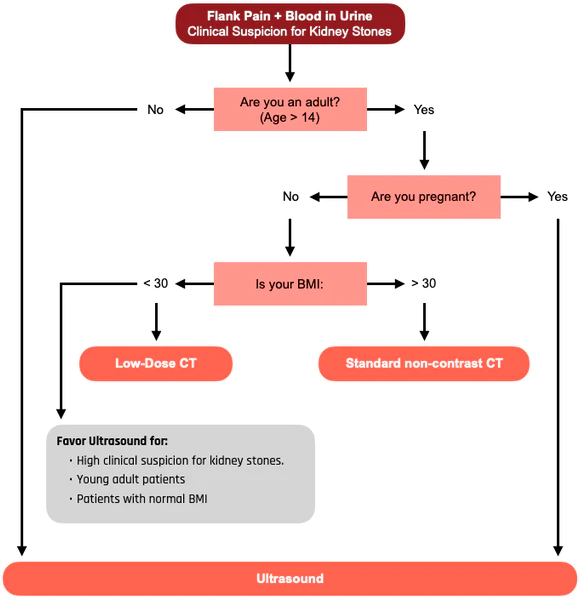
Illustrated graphically, the decision matrix could look something like this as well:
References

Written by Joey Weichmann
Joey Weichmann (aka “The Stone Slayer”) is the Founder of Stone Relief. As an avid naturopath and kidney stone sufferer, Joey has made it his mission to help health-conscious individuals stop kidney stones and get their life back.
Comments or questions?
Responses