Published: February 4, 2024 | 8 mins read
Calcium Oxalate Monohydrate Kidney Stones: Subtypes and Causes
Article Shortcuts
Calcium oxalate stones (CaOx stones) are the most prevalent type of kidney stones globally (80%). These stones are mainly composed of calcium and oxalate ions. Other particles are also present, but these two are dominant.
CaOx stones come in two main forms (known as morphology) based on their internal crystal structure. These forms are known as Calcium Oxalate Monohydrate (Type 1, also called COM stones) and Calcium Oxalate Dihydrate (Type 2, also called COD stones).
Monohydrate kidney stones have five subtypes (Type 1a to 1e), while dihydrate kidney stones have three subtypes (Type 2a to 2c). Some kidney stones may also be a combination of both monohydrate and dihydrate crystals.
In this article, we will discuss in detail the different subtypes of COM stones. But we will cover dihydrate and mixed stones in future blogs.
COM vs. COD Stones
The main difference between these two is their density. Monohydrate crystals are denser than dihydrate crystals. That’s because COM stones have a tighter arrangement of calcium, oxalate, and water molecules, making them denser or harder. In COM stones, each calcium-oxalate crystal holds one water molecule. Meanwhile, in COD stones, each calcium-oxalate crystal has two water molecules. This makes the arrangement of molecules in COM stones more compressed, resulting in higher density. The stronger forces between these closely packed molecules contribute to the firmness of monohydrate stones.
Causes of COM Stones
COM stones are commonly caused by having too many oxalate ions in the urine without a corresponding increase in urinary calcium levels. This high level of oxalate ions is known as hyperoxaluria.
What is Hyperoxaluria?
First, let’s define what an oxalate is. Oxalate is an organic compound found in plants. They are defense chemicals plants use to poison the species trying to eat them. It’s their survival mechanism. That means eating oxalates is harmful.
In fact, oxalates are also called “anti-nutrients.” This is simply because the human body does not possess enzymes capable of metabolizing oxalates. They tend to crystallize in different body parts, causing many diseases, including kidney stones.
The main reason oxalates pile up in our body is inappropriate dietary practices. Eating diets rich in plant matter is the culprit. Again, that’s because almost all plants contain oxalates. Some of the worst foods are spinach, rhubarb, kale, and potatoes. If you want a comprehensive list of oxalate-containing foods, check our Oxalate Content of Foods PDF.
Oxalate levels are considered normal if it’s below 25mg in 24-hour urine. Anything over this number is already high (hyperoxaluric state) and puts you at risk of kidney stones. Read our Hyperoxaluria blog to dig deeper into this topic.
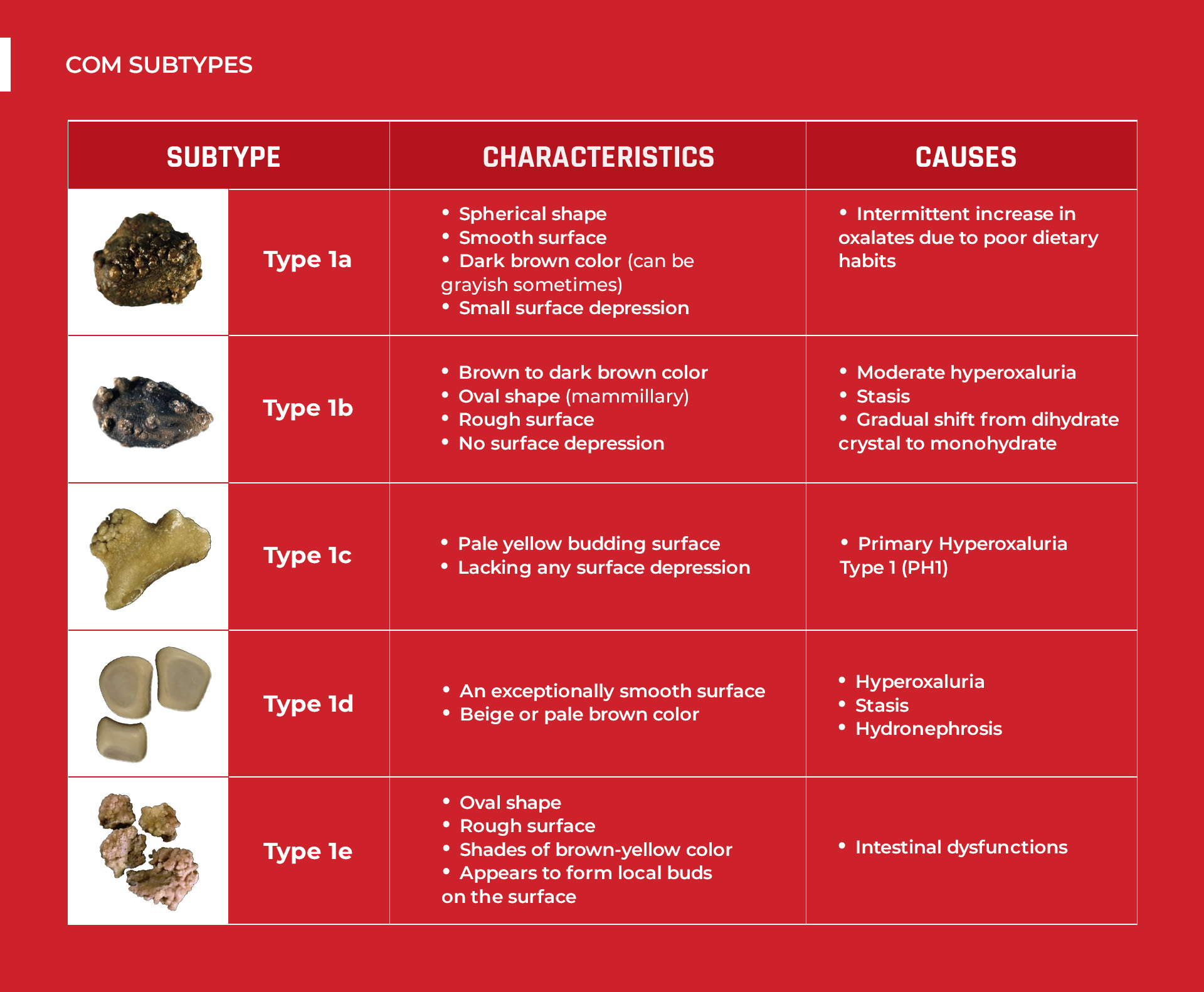
The 5 Subtypes of COM Stones
COM stones have five subtypes, each with a distinct appearance. These distinctions are due to the different ways they form inside the kidney. Let’s look at each of them:

Monohydrate Type 1a Kidney Stones
Type 1a kidney stones are the most common type of kidney stone. These stones are characterized by the following:
Exterior:
- Spherical shape
- Smooth surface
- Dark brown color (can be grayish sometimes)
- Small surface depression
Interior:
-
Compact layers that radiate out from a central point (nucleus)
Interestingly, this structure shows that the formation is linked to intermittent (on again and off again) increases in oxalates due to poor dietary habits. These intervals allow urinary pigments to stick to the crystals. For this reason, most Type 1a kidney stones are dark brown.
Occasionally, the surface of Type 1a stones has very thin and sometimes incomplete white layers made of tiny calcium oxalate monohydrate crystals. Because the underlying layers of crystals are dark brown, the thin superficial deposit appears as a grayish film. These grayish layers indicate a recent spike in hyperoxaluria and suggest an active stage for the stone. Thus, dark brown Type 1a kidney stones are considered dormant or metabolically inactive. By contrast, grayish Type 1a kidney stones are in an active stage.
It’s worth noting that many Type 1a kidney stones show a small depression on the surface (umbilication). This marks the spot where the stone initially formed and attached to the internal structure of the kidney, known as the papilla.

Monohydrate Type 1b Kidney Stones
Type 1b kidney stones are less common compared to Type 1a kidney stones. They have the following characteristics:
Exterior:
-
Brown to dark brown color
-
Oval shape (mammillary)
-
Rough surface
-
No surface depression
Interior:
-
Lacking internal organization
The lack of internal organization in Type 1b stones is due to their distinct formation process. This type forms under moderate hyperoxaluria and when the bladder is not emptying urine fully (also known as stasis). Also, this type will likely form when there’s a gradual shift in crystal composition from dihydrate to monohydrate.

Monohydrate Type 1c Kidney Stones
Type 1c kidney stones typically stem from a genetic condition called Primary Hyperoxaluria Type 1 (PH1). This condition arises at birth and is characterized by insufficient production of a specific enzyme in the liver, leading to excessive oxalate production.
Fortunately, primary hyperoxaluria is extremely rare, affecting only about 3 out of 1,000,000 people. This makes Type 1c stones extremely uncommon.
Type 1c stones consist solely of pure COM crystals. However, they have a distinct appearance:
Exterior:
-
Pale yellow budding surface
-
Lacking any surface depression
Interior
-
Loose and disorganized internal structure
For this reason, Type 1c stones appear very clear on the surface. When examined under an electron microscope, the crystalline structure of typical idiopathic (most probably linked to diet) COM kidney stones differs markedly from kidney stones formed due to Primary Hyperoxaluria Type 1 (PH1). So, when you notice a clear-looking kidney stone like in the image above, it should raise immediate suspicion of Primary Hyperoxaluria Type 1 (PH1) or a condition related to extreme hyperoxaluria.

Monohydrate Type 1d Kidney Stones
Type 1d kidney stones stand out due to their distinct appearance and structure. These are the characteristics:
Exterior:
-
An exceptionally smooth surface
-
Beige or pale brown color
Interior:
-
Having thin concentric layers that lack radiating patterns
Type 1d kidney stones frequently develop in larger quantities, forming when the bladder cannot empty completely (stasis) or when urine backs up in the kidneys (hydronephrosis) within confined cavities. As this type forms in numbers, there’s a tendency for the stones to rub against each other repeatedly. The result is a very smooth and level surface.

Monohydrate Type 1e Kidney Stones
Typically, Type 1e stones are characterized by the following:
Exterior:
-
Oval shape
-
Rough surface
-
Shades of brown-yellow color
-
Appears to form local buds on the surface
Interior:
-
Disorganized with areas of brown-yellow
-
Concentric dark brown layers with a radial arrangement
The primary reason why Type 1e stones form is intestinal dysfunctions. Any dysfunction in the gut affects how nutrients are absorbed. One direct consequence is hyperoxaluria (increased levels of oxalates). Some examples of intestinal conditions that can lead to higher absorption of oxalates in the gut are as follows:
-
Having an inflammatory bowel disease
-
Undergoing small bowel resectioning surgery due to Crohn’s Disease (an inflammatory bowel disease)
-
Children with severe pancreatic deficiency
-
A consequence of bariatric surgery (such as jejunoileal bypass or Roux-en-Y gastrojejunal bypass) for weight loss
Another factor contributing to the formation of Type 1e kidney stones is Type 2 Diabetes. Roughly 6% of kidney stones in diabetic patients display this particular structure. This connection suggests that some individuals with Type 2 Diabetes may develop hyperoxaluria. In fact, a study from 2010 highlighted hyperoxaluria as a risk factor for kidney stones in diabetic patients. It stated that various pathways may convert carbohydrates into metabolic precursors of oxalate, such as glyoxal or glyoxylate. However, more studies are yet needed to prove this connection further.
Preventing COM Stones
As we can see, kidney stones don’t have a one-size-fits-all solution. However, most of them are linked to excessive oxalates in the body. Since hyperoxaluria is mainly of dietary origin, shifting towards a “no-oxalate” diet is necessary. And speaking of no oxalate, we mean rejecting plant foods and going animal-based or carnivore.
Modifying your diet can be challenging. But this is the right thing to do to prevent kidney stones. We suggest replacing plant matter with meat in your diet because animal products are 100% oxalate-free. Even the minority with the genetic condition Primary Hyperoxaluria would benefit from this diet.
There had been disinformation linking protein-rich diets to uric acid kidney stone. This is because of the purine content of protein-rich foods. Our bodies break down purine into uric acid. However, uric acid kidney stones only form on an acidic urine environment (<5.5 pH). Meaning, if you have a neutral urine pH (6.0-7.5), you won’t form this type.
Also, animal-based and carnivore diets don’t lead to health problems like scurvy, indigestion, chronic diseases, and immunodeficiency. These are entirely false and baseless accusations. In fact, these diets are proven safe and effective in preventing most health issues.
If you want to explore the right diet for kidney stones, schedule a coaching call with Joey to clear all misconceptions and discover more about the health benefits of this diet.
Comments or questions?
Responses
You must be logged in to post a comment.

Fact Checked by Joey Weichmann
Written by
The Stone Relief Team
Joey Weichmann (aka “The Stone Slayer”) is the Founder of Stone Relief. As an avid naturopath and kidney stone sufferer, Joey has made it his mission to help health-conscious individuals stop kidney stones and get their life back.
I have been a combo calcium d and m stone maker most of
my adult life. Recently, they changed my diet from little calcium intake to 1200mg from dairy and bok choy, kale,etc. no red meat or chicken, occasional salmon and eggs. Also,, low oxalate diet for many years. I have Randalls Plaque and they say its just inevitable that I will make stones and to drink milk with most
meals as it will allow oxalate to flush and to keep protein at 40g max
(6ft 178lbs) as animal protein will impact my GFR. Issues like kale and animal protein conflict with your messaging. Its all very confusing. I welcome any guidance and opinion that the plaque
prevents me from improving….
Hi John, having Randall’s Plaque alone wouldn’t be a problem if oxalates are not around. We suggest that you read our blog about it to understand Randall’s Plaque more. Also, we have another blog that talks about what really happens if you consume oxalates and calcium within the same meal. Because, many doctors falsely advise this strategy to stone-formers when both calcium and oxalates have different absorption rates. We hope these materials will answer many of your questions. You can find them in the Blog section.
Oxalates are really cumulative. That’s why even a low-oxalate diet is failing most of us. I think it’s best if you can schedule a call with Joey to have him assess your current diet and help you with making appropriate changes.
As always, just shoot us with all your questions in mind.