Published: January 24, 2022 | 1 min read
Expulsive Therapy for Kidney Stones
ARTICLE SHORTCUTS
- EXPULSIVE THERAPY
- MEDICAL THERAPY
- NATURAL EXPULSION
- EXPULSIVE THERAPY AS AN INITIAL TREATMENT OPTION
Expulsive therapy is a relatively new practice in the conservative management of kidney stones that has evolved along with our understanding of the urinary system. Based on this evolution, two paths have evolved to help people pass their kidney stones without the need for surgical intervention. The natural path harnesses centuries-old herbal medicine with other whole foods, while the medical path utilizes pharmaceutical-derived alpha blockers or calcium channel blockers.
EXPULSIVE THERAPY
The goal of expulsive therapy is to help the individual pass their kidney stone in a shorter duration, with less need for analgesic intervention, or for surgical intervention. Prior to the use of either natural or medical expulsive therapies, increased fluid intake, anti-nausea medications, and pain medications were the prescription for kidney stones. Since then, identification of adrenergic receptors in the human ureter and smooth muscle physiology led to the development of targeted medical expulsive therapies. Primarily of the alpha blocker or calcium channel blocker class of drugs.
Before we can fully appreciate the impact of this therapy, we need to understand what happens without an intervention, relying strictly on spontaneous passage:
- 75% of stones < 5mm will pass
- 60% of stones 5-7mm will pass
- 48% of stones 7-9mm will pass
- 25% of stones > 9mm will pass
As you can see, the numbers aren’t that bad. But, they’re not that great, either. That’s where expulsive management comes into play to help increase the passage rate percentage for all kidney stones sizes; especially larger kidney stones. This is why it is oftentimes combined with Extracorpeal Shock Wave Lithotripsy (ESWL). Even through a larger stone has broken apart, the pieces still need to pass. And, expulsive therapy can help make this process smoother.
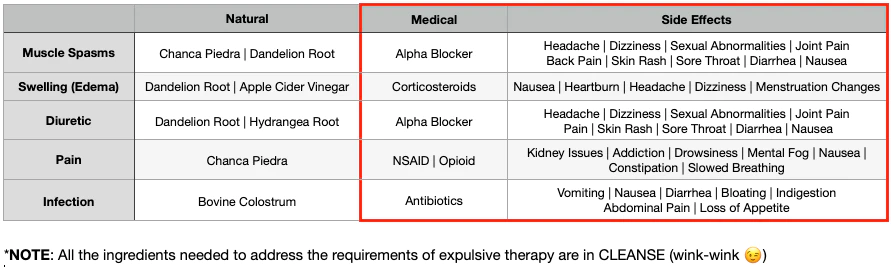
The main factors associated with kidney stone retention include ureteral muscle spasm, submucosal edema (swelling), urine flow, pain and infection within the ureter. As such, any conservative therapy should act on these factors. However, the natural and medical therapy options have differing mechanisms on how to address these factors.
Kidney stones that have moved into the ureter induce ureteral spams. The spasms are believed to stop/slow passage of kidney stones. Corollary to this is that the relaxing of the ureter facilitates passage of kidney stones. Thus, the ureter must be relaxed to help the stone pass faster.
MEDICAL THERAPY
On the medical side of things, there are two different mechanisms by which the ureter can be relaxed. First, Calcium channel blockers work by modifying the effect of calcium on smooth muscle cells of the ureter. This has been proposed to decrease ureteral contractions and renal colic pain.
Second, the ureter contains both alpha and beta adrenergic receptors in varying concentration depending on location in the urinary tract (more dense in distal ureter). Antagonists of the alpha-1-adrenergic receptor inhibit basal tone and decrease peristaltic frequency and amplitude with the added benefit of increased fluid transport and decreased intra-ureteral pressure, they also block the conduction of visceral referred pain to the central nervous system.
The presence of a kidney stone in the ureter also triggers an inflammatory reaction of the mucosa, leading to varying degrees of edema (swelling caused by excess fluid trapped in your body’s tissues). The most frequently used anti-inflammatory drugs in this context are corticosteroids. When given in association with alpha blockers or calcium channel blockers, corticosteroids will decrease edema and inflammation; thereby eliminating an obstacle to the passage of the kidney stone. Antibiotics and analgesic therapy complete the medical expulsive regimen.
NATURAL EXPULSION
The natural side is a lot less complicated even though it deals with the same underlying mechanisms (ureteral spams, swelling, and pain). Natural anti-inflammatories such as Chanca Piedra and Dandelion Root can aid in relaxing the ureter and in reducing inflammation that restricts kidney stone movement. Natural diuretics can increase urine flow which will aid in faster stone passage when combined with the freedom of movement created by the anti-inflammatories.
Individuals with certain weaker density kidney stones such as Calcium Oxalate Dihydrate, Cystine, and uric acid will also benefit from the anti-lithic nature of the natural expulsive path. Many of the herbal and whole food based ingredients used in natural therapy for kidney stones act as anti-lithic or “stone-breakers.” If you have these weaker kidney stone types (learn more here), you may be able to break apart the larger stone before it has a chance to pass whole with a product such as CLEANSE.
EXPULSIVE THERAPY AS AN INITIAL TREATMENT OPTION
Despite all of it’s advantages, expulsive management is rarely used. This represents a failure of the translation of medical science into practice. A study performed by Hollingsworth et. Al. reported that the overall prevalence of medical expulsive therapy in emergency departments in the USA was 1.1%.
This is a missed opportunity of sparing roughly 260,000 individuals annually from kidney stone surgery. It really shows you the state sad that we’re in when it comes to healthcare.
If faced with a new diagnosis of a kidney stone in the ureter of less than 10mm without indications for immediate surgical intervention (such as uncontrolled pain, inadequate kidney function, or clinical evidence of sepsis), we would highly recommend an initial treatment option of observation with periodic evaluations. By adding expulsive therapy to this, stone expulsion may be achieved during the observation period.
REFERENCES:
1. Outcome of uncomplicated ureteric calculi managed with medical expulsive therapy in the outpatient clinic of a urology unit in Sri Lanka
2. Medical expulsive therapy
3. Guideline of guidelines for kidney and bladder stones
4. Management of ureteral calculi and medical expulsive therapy in emergency departments
5. The use of alpha-blockers for the treatment of nephrolithiasis
6. Medical expulsive treatment in pediatric urolithiasis
7. Current use of medical expulsive therapy among endourologists
8. Medical expulsive therapy for ureteric stones: Analysing the evidence from systematic reviews and meta-analysis of powered double-blinded randomised controlled trials
9. Update on medical expulsive therapy for distal ureteral stones: Beyond alpha-blockers

Written by Joey Weichmann
Joey Weichmann (aka “The Stone Slayer”) is the Founder of Stone Relief. As an avid naturopath and kidney stone sufferer, Joey has made it his mission to help health-conscious individuals stop kidney stones and get their life back.
Comments or questions?
Responses