Published: May 19, 2024 | 9 mins read
Medullary Sponge Kidney Can Lead to Calcium Phosphate Stones!
When we began our journey into kidney stone research, we met many people suffering from medullary sponge kidney disease (MSK) and recurrent kidney stones. So, we joined FB groups and other communities that would help us understand what this condition is really about and how it affects kidney stones, particularly calcium phosphate stones.
We realized that there is a connection between these two conditions that we need to understand on a deeper level. According to the statistics, 70% of MSK patients form kidney stones, and 12% to 20% of kidney stone-formers have MSK.
Unfortunately, most doctors just prescribe thiazide diuretics for MSK patients to help them have a continuous urine flow, and that’s all. No action plan to prevent kidney stones whatsoever.
This is more than frustrating.
That’s why we took the initiative to write this blog, which we know will benefit many kidney stone-formers.
Before we dig deeper into MSK and kidney stone connection, let’s first discuss what medullary sponge kidney disease is about.
What is Medullary Sponge Kidney Disease?
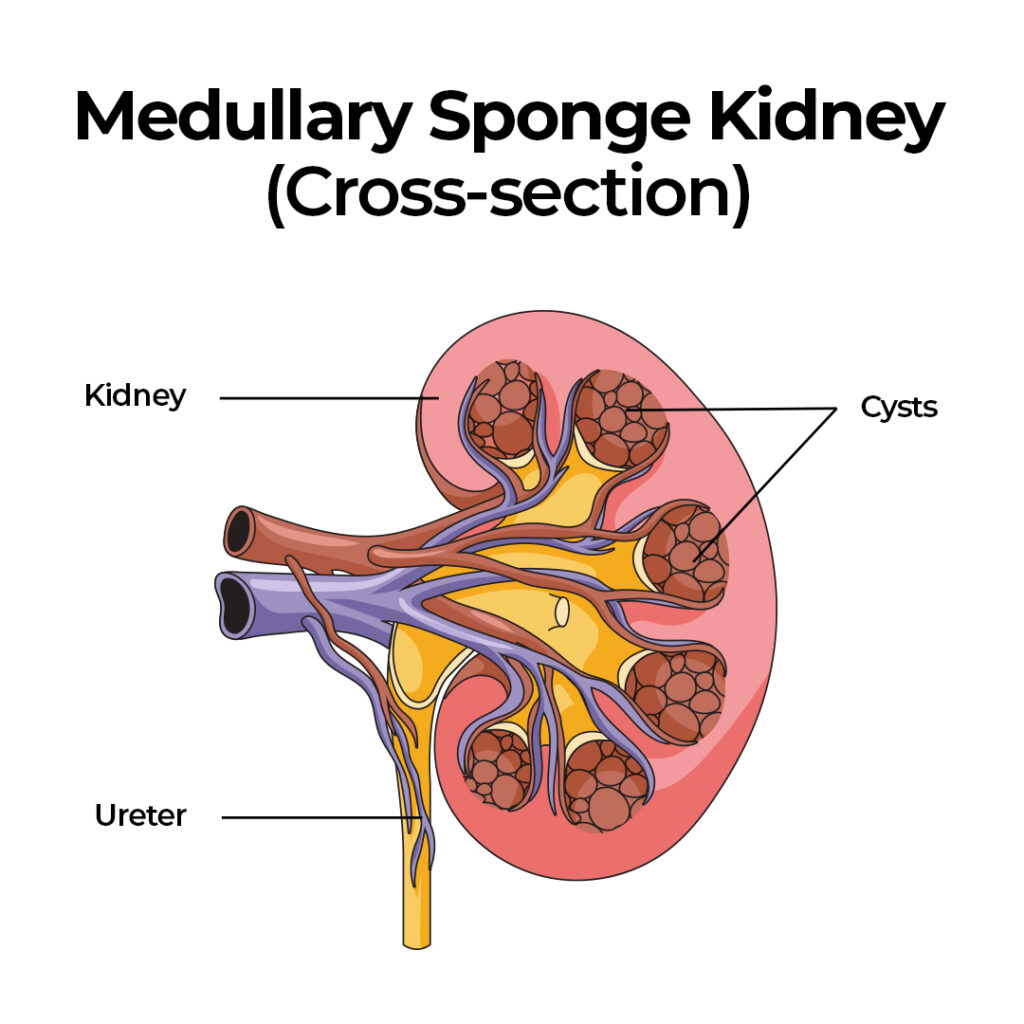
Medullary sponge kidney is a rare congenital disorder, meaning it’s present from birth. It happens when tiny sacs, called cysts, form on the small tubes inside the kidney (tubules) or on the collecting ducts, which gather urine for elimination. During fetal development, they form within the inner part of the kidney called the medulla. These cysts can affect one or both kidneys and restrict urine flow.
These multiple small cysts vary in size from 1 mm to 8 mm, making the kidney look like a sponge when cut, which is how it got its name.
Medullary sponge kidney symptoms usually appear in the teenage years or the 20s. It usually presents itself through the following:
- Hematuria
- Recurrent kidney stones
- Urinary tract infections (UTIs)
MSK rarely leads to severe problems, such as chronic kidney disease or kidney failure. However, recurrent kidney stones do! So, it is essential to stop recurring kidney stones in MSK patients.
But how is medullary sponge kidney disease connected to kidney stones exactly?
We’ll dive into this critical question in the next chapter.
Medullary Sponge Kidney and Kidney Stones
Medullary sponge kidney disease is rare. Only about one in 5,000 people has it. However, if you have this condition, it often leads to recurrent kidney stones, particularly calcium phosphate stones. Usually, it comes with severe kidney stone pain and blood in the urine. It can also trigger urinary tract infections (UTIs), worsening the situation.
There are two main reasons why MSK affects your kidney stone risk:
Urine flow obstruction
Due to structural abnormality in the kidneys of those people with MSK, they often struggle with stagnant urine flow. Stagnant urine is the playground of stone-forming elements waiting for the chance to bind together, form stones, and cause you enormous pain!
Yes, MSK patients often struggle with severe urine backup in their kidneys (hydronephrosis) and extreme kidney stone pain.
If this is your current condition, using CLEANSE can alleviate the pain and encourage better urine flow. If a stone is lodged somewhere in your urinary tract, CLEANSE will also help pass that stone out.
Okay, if you think urine backup is already bad, the next section will tell you something worse that MSK can cause.
Distal Renal Tubular Acidosis (dRTA)
Have you ever played a “Plinko” game? If you’re unfamiliar with this game, you typically drop a ball down a vertical board with pegs and obstacles. That ball lands in slots at the bottom. This is the same logic with MSK. Your kidney has those obstacles, so it faces many difficulties.
When you have MSK, your kidneys might experience problems concentrating urine and excreting acid properly. This can result in a condition known as distal renal tubular acidosis (dRTA).
Having dRTA is like losing all your aces in a card game. It can cause three risk factors for kidney stone formation:
1. Alkaline urine (over 7.0 PH)
When the kidney has trouble excreting hydrogen ions in the urine, it becomes more alkaline than usual. Alkaline urine favors calcium binding with phosphate instead of oxalates.
Aside from alkaline urine, dRTA causes another trouble – low citrate levels.
2. Low urinary citrate
If you have read our previous blogs, you know we’ve been comparing citrate to Ironman’s armor. Citrate shields calcium against any stone-forming elements, such as oxalates and phosphate, that try to stick to it.
However, if you have dRTA, you lose the opportunity to shield yourself. Again, when you have dRTA, your kidneys fail to excrete acid into the urine. That means your blood becomes acidic. So, to buffer your blood’s acidity, your kidneys will reabsorb citrate back into the bloodstream. Imagine expecting a very important parcel delivery because you need it right now, or you’ll lose a million-dollar business deal. Then suddenly, the delivery guy received an emergency call because his mom was on her deathbed. Instead of completing the delivery, he turned around and left. Will you get mad?
In dRTA, your kidneys are in that critical decision-making phase, and they choose to send citrate back where it’s more needed – in the blood.
But wait, we’re not yet done with dRTA. There’s still another reason why it’s troublesome for kidney stone-formers…
3. Increased urinary calcium levels
When the kidneys cannot properly excrete hydrogen ions into the urine, acid buildup in the blood can occur. This acid buildup can strip calcium from bones, increasing calcium levels in the urine.
Although calcium is NEVER the main reason for stone formation, it will pose a problem if you have stone-forming materials floating in your urine due to eating plant-based diets!
You are probably thinking right now – how the hell does a person develop medullary sponge kidney disease?
If you want the answer, hang tight; we’ll get there in the next section.
Medullary Sponge Kidney Causes
Doctors don’t know the exact cause of medullary sponge kidney disease. And though it’s congenital (present at birth), there’s no evidence that it is hereditary.
While some instances are believed to have familial links, no specific genetic basis has been identified, and it’s generally not considered hereditary except in around 5% of cases that follow a genetic pattern.
What about the 95%?
While scientists claim that the exact cause of MSK is unknown, we have a theory that it is related to calcium deficiency during pregnancy.
Why do we say that?
Some research hints at a possible link between hyperparathyroidism and this kidney condition. Hyperparathyroidism means that your parathyroid glands (four small glands in the neck area) produce too much parathyroid hormones (PTH). PTH helps regulate calcium levels in the body. This condition is highly connected to long-term calcium deficiency.
Also, vitamin D and vitamin A toxicity due to long-term intake of synthetic supplements can badly affect your parathyroid glands.
Remember, medullary sponge kidney disease is NOT hereditary. You can develop it while you are still in your mom’s womb. But it’s entirely up to you how you take our hypothesis.
Anyway, here are the genetic conditions that could be causing the 5% of MSK cases:
- Beckwith-Wiedemann syndrome – Characterized by overgrowth, abdominal wall defects, large organs, and an increased risk of certain cancers.
- Wilms tumor – A type of kidney cancer that primarily affects children, arising from immature kidney cells
- Horseshoe kidney – The kidneys’ lower ends are fused across the midline, forming a horseshoe shape.
- Rabson-Mendenhall syndrome – Characterized by severe insulin resistance, abnormal growth, and other developmental abnormalities.
- Cakut syndrome – A group of birth defects affecting the kidneys, ureters, bladder, and urethra, leading to urinary tract abnormalities.
- Polycystic renal disease – Characterized by the formation of fluid-filled cysts in the kidneys
- Caroli’s disease – Characterized by the presence of cysts in the liver’s bile ducts
Suppose you suspect that you might have MSK. In that case, you can take any of these imaging modalities to confirm whether you really have this condition:
- Intravenous Pyelogram (IVP) – A contrast dye is injected into the vein
- Computerized Tomography (CT)
- Ultrasound
Let’s say you confirmed that you have medullary sponge kidney disease. Is there a way to cure this condition? And how do you prevent your child from developing MSK? If you want answers to both questions, hop into the next section.
Manage and Prevent Medullary Sponge Kidney
Unfortunately, medullary sponge kidney in adults has no cure. Once you confirm that you have this condition, all we can do is manage it to prevent serious complications.
Since MSK is highly related to recurrent kidney stones and also UTIs due to stagnant urine, treatment is directed to these two areas.
If you currently have kidney stones, use CLEANSE to pass all your stones with less pain. MSK patients often experience extreme kidney stone pain due to their kidneys’ structure. CLEANSE provides so much relief in that area because it has pain relief, anti-inflammatory, diuretic, and stone-dissolving properties.
It is critical for stone-formers to fix their diet. They need to stop eating plant-based foods and eat more animal-based foods. Stone-forming elements can get trapped in the little pockets in your kidneys and form stones! This goes the same way for expecting mothers. Stop eating plant-based foods and go animal-based. An animal-based diet will not leave you calcium-deficient.
A nice, even, consistent daily hydration is also advisable to prevent severe urine backup.
If you need more granular advice on managing or preventing medullary sponge kidney and kidney stones, check out our Coaching Program. This will give you an opportunity to ask questions and formulate a personalized plan based on your situation.
REFERENCE:




Fact Checked by Joey Weichmann
Written by
The Stone Relief Team
Joey Weichmann (aka “The Stone Slayer”) is the Founder of Stone Relief. As an avid naturopath and kidney stone sufferer, Joey has made it his mission to help health-conscious individuals stop kidney stones and get their life back.
I have some questions about nephrocalcinosis.
Hi @cruzirene91yahoo-com , you’re in the right place 🙂 What questions can we answer for you?