Published: January 31, 2022 | 23 mins read
Shockwave Lithotripsy (SWL) for Kidney Stones
Shockwave Lithotripsy (SWL) was first used to treat kidney stones in 1980. This treatment modality uses sound waves to break apart kidney stones so that smaller fragments may pass through the urine. In the 40+ years since its introduction, SWL has become widely popular and is currently one of the first-line options for the non-invasive treatment of kidney stones less than 20mm in diameter without the requirement for general anesthesia. However, due to its incredibly complicated nature and unreliable performance, alternative treatment methods with higher success rates are becoming more prevalent.
INTRODUCTION
With technological advances in the field of endoscopy (Ureteroscopy) and the inconsistent results of Shockwave Lithotripsy (SWL), the procedure has been on the decline for the last decade. As you will observe through this blog, SWL can be a complicated procedure when it comes to patient selection. Additionally, from the patient side of things, multiple procedures are frequently required putting a toll on them physically and financially.
However, it’s important to note that repeated treatment sessions may be necessary within the scope of this procedure and that this should not be considered a failure – instead, simply a consequence of the physics relating to non-invasive kidney stone disintegration.
NOTE: It is essential to discuss your openness to multiple procedures with your Doctor if Shockwave Lithotripsy (SWL) is your preferred treatment method.
There may be practitioners who will attempt to use excessive shockwaves and/or unnecessarily high and risky energy levels to complete the procedure in one session. If you are not open to multiple SWL procedures and the kidney stone cannot be passed with Expulsive Therapy, endoscopic procedures are your best alternative.
While experience has shown that complications after EWSL are lower than that of endoscopic procedures and open surgical procedures, particular attention must be paid to the risk of developing:
- Renal sub capsular hematoma
- Other types of trauma to the kidney
- Injuries to surrounding organs
- Problems associated with infected urine or kidney stones
- Urine flow obstruction caused by stones and fragments
PATIENT SELECTION
Successful treatment with Shockwave Lithotripsy (SWL) cannot be realized without appropriate patient selection. Radiological imaging is a critical component that allows medical professionals to identify several other necessary morphological features. Kidney stone size (longest diameter, stone surface area, or stone volume), stone location, and stone density in Hounsfield Units should be determined (learn more about kidney stone density here). This information aids in roughly predicting a success rate and the need for repeated sessions or other necessary precautions.
There are few absolute contraindications for Shockwave Lithotripsy (SWL). Individuals who are pregnant or suffer from uncorrected coagulation disorders should not be treated with SWL despite occasional reports in the literature. Additionally, individuals with Ureteropelvic Junction (UPJ) obstruction, ureteral strictures, or any other anatomical abnormality that will hinder fragment passage should not be treated with SWL. The only exception to this rule is when the treatment plan includes combined procedures such as SWL and Percutaneous Nephrolithotomy (PCNL). Skeletal deformities (such as severe scoliosis) might also make SWL impossible.
Particularly attentive care is strongly recommended for patients with specific risk factors. The most important of these conditions are summarized below:
- Hypertension
- Borderline blood pressure (~140/90 mmHg)
- Patients treated for hypertension
- Cardiovascular disease
- Diabetes mellitus
- Reduced renal function
- Children
It is imperative to avoid over-treatment in patients with these conditions – both in terms of shockwave energy and the number of shockwaves. The rule is that it is always better to retreat than to expose the patient to unnecessary risk of bleeding or tissue trauma.
Individuals with multiple kidney stones are poor candidates for Shockwave Lithotripsy (SWL). The same is true for staghorn stones. This is because the residual stone fragment volume is too high and often overloads the urinary tract, leading to complications. The only exception to this rule is when SWL is combined with PCNL surgery.
The maximum size kidney stone that Shockwave Lithotripsy (SWL) can impact varies from facility to facility. However, it is generally considered a good choice for stones in the kidney (not in the ureter) with maximum diameters up to 20mm (stone surface average~200-225 mm^2). This can be expanded up to 30mm for kidney stones with low density (see list of stone types here)
It’s important to note that Shockwave Lithotripsy (SWL) is also not suggested for kidney stones larger than 15mm located in the kidney’s lower calyx. Some have even suggested an upper stone size limit of 10mm for lower calyx stones. This is because most of the residual fragments post-procedure end up collecting in the lower calyx, making expulsion more difficult.
Decisions to treat large and very dense (> 850 HU) kidney stones with Shockwave Lithotripsy (SWL) requires careful consideration of the individual’s stone situation, risk factors, and personal preferences. If your Doctor is considering this treatment option for a kidney stone larger than 20mm, it is wise to exclude the following stone types:
- Brushite
- Calcium Oxalate Monohydrate
- Cystine (very compact)
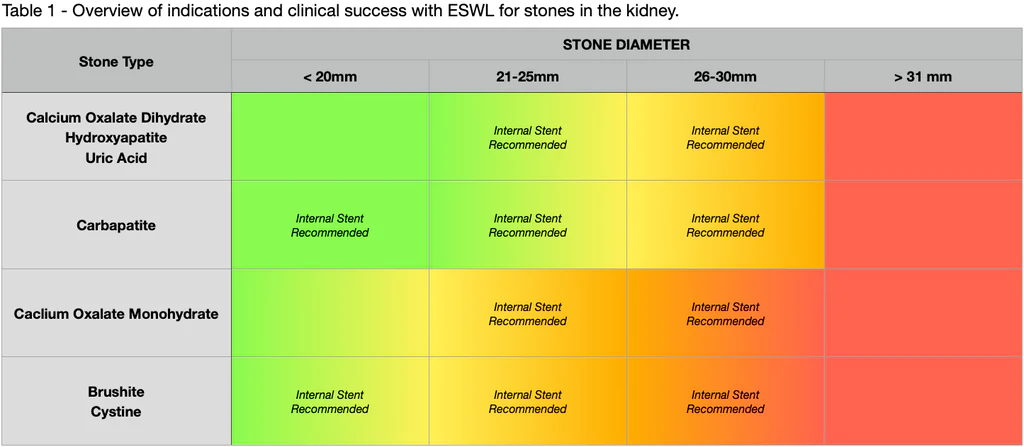
To translate all of these patient selection criteria into a more user-friendly format, please see Table 1 below. Table 1 represents clinical success for treating stones located in the kidney. Here’s what the different colors mean:
???? Stone is suitable for SWL
???? SWL is an option. But, individuals will require multiple treatments
???? SWL should be a secondary treatment option to another procedure type
???? Stone is NOT suitable for SWL
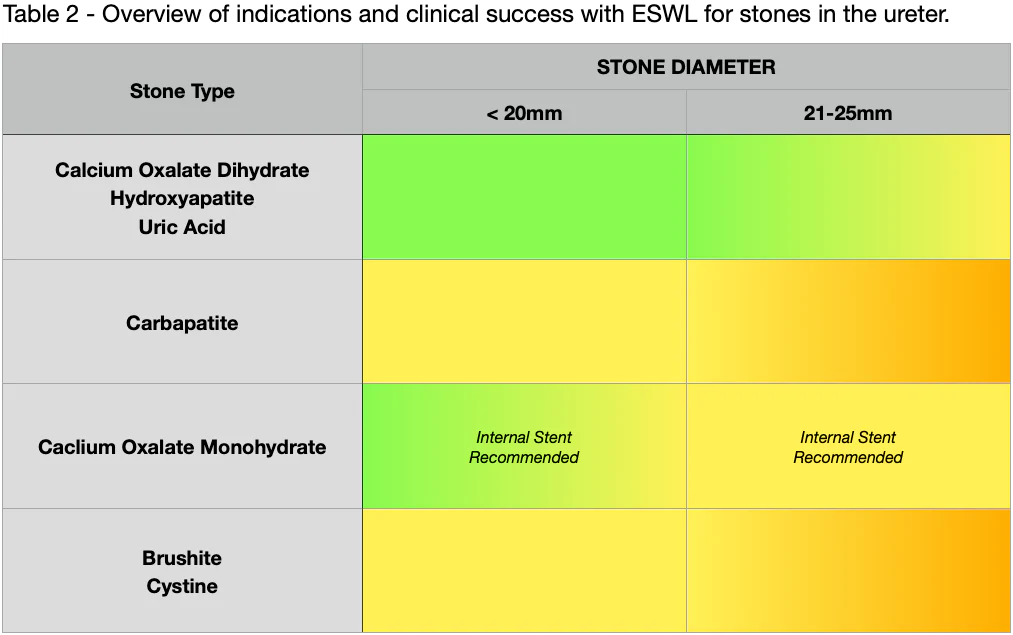
When considering using Shockwave Lithotripsy (SWL) to treat kidney stones in the ureter, Table 2 below will provide an overview of indications and estimated clinical success, just as with Table 1 above. As you can see, stones at all locations in the ureter are good candidates for SWL. Some suggest a diameter limit for stones in the upper ureter of 10mm. However, it has been repeatedly demonstrated that larger stones can also be treated with favorable results.
Kidney stone density plays a significant role in determining candidates for Shockwave Lithotripsy (SWL). As discussed in previous blogs, kidney stone density is represented in Hounsfield Units (HU) (learn more about kidney stone density here). In addition, numerous studies indicate an inverse relationship between stone density and stone fragmentation capabilities with SWL (i.e., the denser the kidney stone, the less likely it will fragment).
If an individual has a recent kidney stone analysis or CT scan, this information can be precious. Even if the density information from a CT scan is from the past, it can still be helpful. This is because kidney stone types rarely change over a person’s lifetime (except if significant changes to diet/lifestyle have been intentionally undertaken- which would merit re-imaging).
The most shockwave-resistant kidney stone types are Calcium Oxalate Monohydrate, Brushite, and Cystine. Like Calcium Oxalate stones, Cystine comes in two different variations. One is less dense and susceptible to Shockwave Lithotripsy (SWL), and the other is very dense and is resistant to SWL. It is important to note that while these stones are more difficult to destroy than other weaker density stones, they can still be eliminated with SWL, provided appropriate energy levels and repeated sessions are acceptable.
When it comes to using stents, the general rule of thumb is to use them before treating kidney stones larger than 20mm in the kidney. In addition, a stent is generally not applicable if a stone is located in the ureter unless there is a pronounced obstruction. Several observational studies have demonstrated that a stent can negatively impact SWL performance when treating stones in the ureter.
Another factor that needs to be considered when determining selection criteria for Shockwave Lithotripsy (SWL) is obesity. With nearly half the population in the United States having a BMI over 30, this creates a unique challenge for medical professionals and patients alike seeking non-invasive treatment options for kidney stones. Unfortunately, when it comes to SWL, a BMI of over 30 creates too much distance between the kidney stones being treated and the head of the machine where the shockwaves are emitted. With this limited penetration depth, stones cannot be appropriately placed in the shockwave focus. There is also considerable energy loss when the shockwaves hit abdominal fat and muscle tissue
Thus, when evaluating Shockwave Lithotripsy (SWL), something called Skin-to-Stone Distance (SSD) must be considered. Distances of more than 100-110mm and a kidney stone density exceeding 850 HU significantly reduce the effectiveness of SWL. However, it is sometimes possible to overcome this limitation with obese patients using an extended shockwave technique called “blast path.” Higher energy levels may also be required to achieve success in these individuals.
TREATMENT TIMING
Early intervention with Shockwave Lithotripsy (SWL) has been reported to field a higher success rate when compared to delaying SWL. However, early treatment for kidney stones less than 10mm may represent an over-treatment because many of these stones will pass spontaneously or with the application of Expulsive Therapy (learn more about expulsive therapy here). Table 3 outlines success rate percentages based on when SWL treatment was sought.
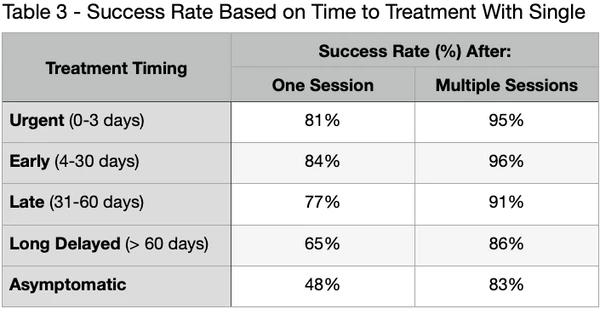
As you can see, asymptomatic individuals (no signs of renal colic or other symptoms) and people in the long-delayed groups had lower success rates when compared to those in the urgent and early groups. Additionally, success rates after multiple Shockwave Lithotripsy (SWL) sessions were lower for kidney stones greater than 10mm in diameter than for stones less than 10mm in diameter.
NOTE: It is essential to seek SWL treatment within 60 days of symptom onset for the best results.
REDUCING RISK & INJURIES
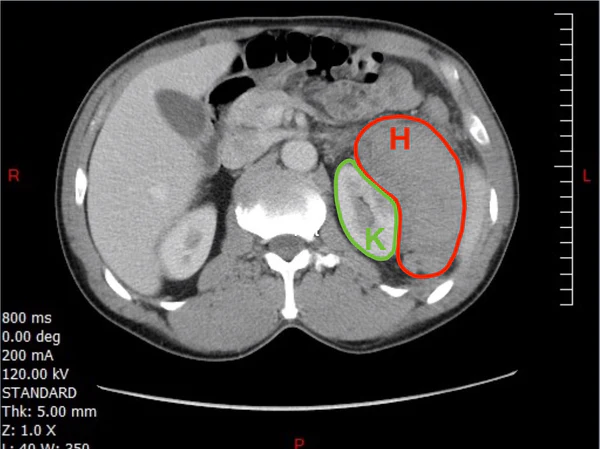
One of the most serious and feared complications of Shockwave Lithotripsy (SWL) is the development of renal subcapsular hematomas. The picture below illustrates what happens in this complication (the “H” is the kidney and “K” is the subcapsular hematoma). The blood loss and effects on renal function are severe. Fortunately, this complication is pretty rare (~1% of procedures).
Individuals with high blood pressure have an increased risk for this complication. As mentioned previously, your Doctor needs to identify all the major risk factors when considering SWL. If hypertension is identified, the pressure should be normalized before shockwaves can be applied. The same restrictions are necessary for any SWL treatment that runs the risk of hitting any renal tissue with shockwaves. It is particularly important when treating kidney stones located in the upper ureter. Stones in the middle or lower ureter are not a problem in this regard.
Another potential form of complication is macroscopic hematuria. This bleeding is a consequence of injuries to the urinary tract lining caused by kidney stone fragments tearing the mucosa. However, it is important to note that without an episode of macroscopic bleeding, the stone was likely not destroyed. So, if the SWL procedure is not accompanied by hematuria, the treatment variables should be adjusted, or the stone position in the lithotripter reconsidered. You take a little good with the bad in this instance.
NOTE: Individuals on anti-platelet treatment of any kind are at significant risk of bleeding complications, and treatment should not be performed until this risk has been eliminated. This is also true for individuals on anticoagulation treatment with Warfarin or similar drugs. Endoscopy is often the best alternative for these high-risk individuals.
When it comes to the actual application of Shockwave Lithotripsy (SWL), several studies have demonstrated that shockwaves administered at a low rate generate much less pronounced injuries to the kidney. This is particularly important to consider when evaluating treatment eligibility for individuals with an increased risk of bleeding or renal injury. In addition, with the administration of a slow rate shockwave, it is possible to avoid or decrease the adverse effects of cavitation bubbles that remain in the tissues at the time of the next shockwave.
Most investigations into shockwave rates have been made between the frequencies of 120 and 60. However, whether a frequency of 60 is better than 90 has not been established. On the other hand, it has been shown that frequencies as low as 30 produce even more minor tissue injury. Thus, for individuals with specific risk factors, a slow rate of shockwave delivery is recommended.
The destruction of kidney stones using Shockwave Lithotripsy (SWL) always results in contusions. Therefore, it is wise not to repeat treatment until a sufficient recovery period has been established (typically 10-14 days). Calcium channel blockers have been shown to decrease injuries too.
Lastly, occasional organ-related complications such as acute pancreatitis and damage to the pancreas, spleen, liver, lungs, and intestines have been reported. Fortunately, these are all pretty rare. Another question that comes up often is whether or not SWL impacts our reproductive organs. Fortunately, here again, both animal models and clinical experience have shown that SWL can be carried out close to the ovaries and testicles without risk of injury.
INFECTION COMPLICATIONS
The second significant risk of complications with Shockwave Lithotripsy (SWL) is bacteria. Bacteria are present in your urine and potentially in your kidney stone and can be released during the destruction of your stone with SWL. With the resulting obstruction to urine flow caused by stone fragments after the procedure, life-threatening septicemia and septic shock can emerge. Therefore, it is critically important to identify infection risks before SWL. As such, it is a mandatory requirement that all individuals are tested for bacteria before treatment.
If the test comes back positive, Your Doctor should add a urine culture for subsequent treatment with antibiotics. However, even if the test comes back negative and bacteria have not been identified, it is unfortunately still necessary for antibiotics to be used, especially for individuals with a history of urinary tract infections (UTI).
MANAGING OBSTRUCTIONS
Destruction of kidney stones should always result in fragments that will be eliminated through the ureter. However, the accumulation of impacted fragments in the ureter can cause obstructions. This condition is called “Steinstrasse,” and it increases with initial stone volume (i.e., the larger the stone, the more incidence of Steinstrasse). In most cases, both isolated stone fragments and “Steinstrasse” can be treated and eliminated with repeated Shockwave Lithotripsy (SWL) procedures.
To avoid the problem of obstruction caused by large kidney stone fragment volumes, internal stents are often inserted before the procedure. Stents are recommended for stones with a diameter exceeding 20mm. There are, however, many reports in the literature indicating that stenting is not necessary. So, you may experience variability from one practitioner to another concerning the use of stents. Stenting can also be recommended for weakened individuals where an obstruction might cause harm.
NOTE: Children’s ureters are much more flexible and transport a much higher capacity kidney stone fragment load than adults. Thus, the use of stents can be omitted in most children.
When an obstruction in the ureter is also associated with impaired renal function and/or infection, inserting a stent or nephrostomy tube is mandatory before any additional procedures. In case of infection, antibiotics should be started immediately.
Because of the nature of this procedure creating kidney stone fragments from the destroyed stone, Shockwave Lithotripsy (SWL) is often combined with Expulsive Therapy to help the fragments pass with less complication. It is your choice to either accept Medical Expulsive Therapy (MET) using pharmaceuticals that may be prescribed by the Hospital performing your procedure or to utilize Natural Expulsive Therapy (NET). Suppose you want to avoid the litany of adverse side effects associated with MET. In that case, we recommend Natural Expulsive Therapy with a product like CLEANSE (learn more about CLEANSE here). Either option is suitable for assisting with residual fragments from SWL.
NOTE: Traditionally trained Urologists & Doctors will likely not recognize Natural Expulsive Therapy (NET). However, this has little to do with NET’s efficacy. Instead, it merely reflects the limited exposure to naturopathic medicine for most Western Medical professionals.
PACEMAKERS & DEFIBRILLATORS
Shockwave Lithotripsy (SWL) can treat individuals with pacemakers or defibrillators. However, there may be specific devices disturbed by the electromagnetic field of shockwaves. Therefore, your Doctor should consult the responsible cardiologist before treatment if you have one of these medical
TECHNICAL ASPECTS
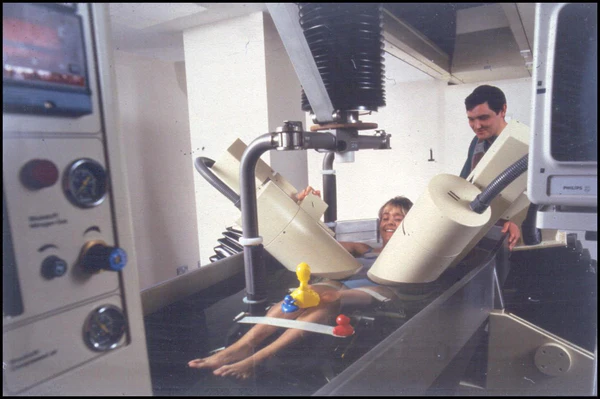
The fundamental requirement for successful Shockwave Lithotripsy (SWL) is that the shockwave can pass into the body and hit the kidney stone with minimal energy loss. The original lithotripter introduced back in the 1980s generated shockwaves in the same compartment as the patient (see photo below). Modern lithotripters have a gap between the shockwave source (therapy head) and the body that needs to be bridged. This gap is usually bridged with a transmission medium such as ultrasound gel or silicon oil.
It is vital to avoid the simultaneous creation of air bubbles when the retransmission medium is applied to the therapy head. Additionally, the presence of even small volumes of air between the therapy head, transmission medium, and the body will reduce the effectiveness of the procedure and, in the worst case, completely extinguish the energy from the shockwave. Therefore, optimal coupling of the therapy head and body is imperative and why a very liberal transmission medium is often applied.
The following steps in the Shockwave Lithotripsy (SWL) procedure involve identifying the kidney stone target and positioning the patient. Fluoroscopy is most commonly used. But, Ultrasound is another option. Especially when trying to target radiolucent stones such as uric acid, which are not visible on X-Ray (learn more about imaging here). The current recommendation is to use the pulsed technique of Fluoroscopy to reduce radiation load. However, continuous Fluoroscopy may be used with individuals where respiratory movements are negatively impacting the procedure results.
Fluoroscopy is a medical procedure that makes a real-time video of the movements inside a part of the body by passing x-rays through the body over time. X-rays are a form of ionizing radiation.
The success rate of Shockwave Lithotripsy (SWL) correlates directly with Fluoroscopy time. However, it is crucial to keep the radiation load as low as possible through collimators early in the SWL treatment to reduce the radiation field maximally. If this is neglected, you may be presented with unnecessarily high doses of radiation. For example, the radiation dose with a wide-open aperture is approximately 20x higher than that following collimation of the aperture to a square 7×7 cm.
Collimator: a device that narrows a beam of particles or waves. To narrow can either cause the direction of motion to become more aligned in a specific direction (i.e., make collimated light or parallel rays) or cause the beam’s spatial cross-section to become smaller (beam limiting device).
With the kidney stone in focus, it is vital to ensure no skeletal structures in the shockwave path. For example, with the delivery of shockwaves from the back of the patient, interference might be caused by small bony projections off the right and left sides of each vertebra called transverse processes, the ribs, and different parts of the sacroiliac bone and pelvic skeleton.
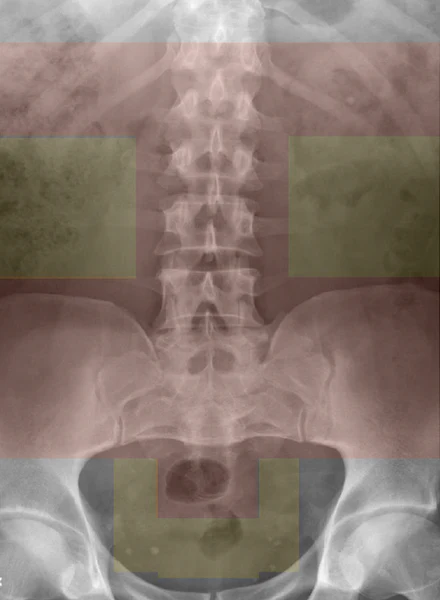
The picture above indicates the different zones in this regard. Here’s what the different colors mean:
???? SWL can be conducted with shockwaves directed from the back
???? SWL can be conducted with shockwaves directed from the front
Kidney stones located between the spine and pelvic brim are a common problem. The skeleton in this area has a considerable ability to absorb energy. Stones just below the sacroiliac joint suffer from similar issues. See the photo below to get an idea of where these issues occur physically in relation to your body.
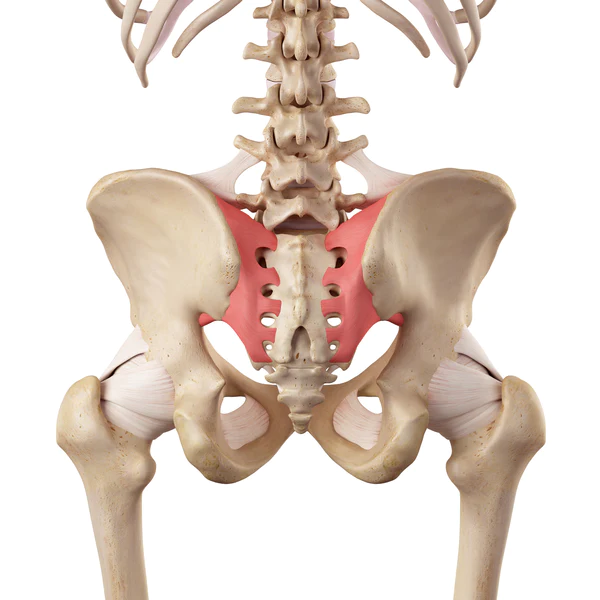
Adjustments to your position will, in most situations, solve the problem and allow for shockwave administration from behind. However, if adjusting your position is not possible, shockwaves can be administered from the abdominal side (front). Applying shockwaves from the front is always necessary with kidney stones located in the middle ureter and is sometimes elected for stones in the lower (distal) ureter.
Applying shockwaves from the abdominal region is interference with intestinal gas. No treatment should be carried out when gas is found in the shockwave path. The gas will completely extinguish the shockwave energy and increase the intestinal wall’s risk of trauma. Gas can be eliminated with an enema and occasionally with a massage.
Animal models and clinical experience have shown that the risk of tissue injury with bleeding can be reduced by “ramping” the shockwaves. This works by using a low energy level (for instance, 100 shockwaves) at the onset of the procedure and slowly ramping the energy level up throughout the procedure. Ramping has several advantages:
- Easier for awake patients to adjust to the treatment
- Identifies at which energy level kidney stone destruction begins to avoid over-treatment in terms of energy.
Moreover, several research studies have indicated that ramping results in better kidney stone destruction than when power is rapidly increased to high levels or when a high power level is constantly used during the procedure. It is also important to note that high energy levels equate to larger fragments, and lower energy levels result in smaller fragments.
Excessive shockwaves during a single session may result in contusions or other tissue damage. Therefore, it is essential that Doctors don’t over-treat individuals in terms of both shockwave numbers and shockwave energy levels. The most commonly recorded upper limit for shockwaves in a single session is 2000-4000 (adjusted for total energy applied). Treatment should be stopped when sufficient kidney stone destruction has been achieved. For individuals with specific risk factors (identified earlier in this blog), a low number of shockwaves and ow energy levels should be used. The same principles should be applied to children.
Unfortunately, it is not possible to give a specific recommendation regarding the total number of shockwaves. Kidney stone size and density and your body’s unique features will influence these factors. However, it is essential to note that the treatment should be stopped if a stone has not been adequately destroyed after 3000-4000 shockwaves. A subsequent procedure can be scheduled after an adequate rest period to finish the work.
Clinical and experimental studies have indicated that 60 (1 Hz) shockwave frequency is better than 90 (1.5 Hz). However, a 60 (1 Hz) frequency should be used for individuals with specific risk factors or children.
ELDERLY PATIENTS
Since its conception, urologists have used shockwave Lithotripsy (SWL) as a first-line treatment option for uncomplicated kidney stones in elderly patients. Despite changes associated with aging and the likelihood of other medical issues, SWL is safe and well-tolerated in the elderly population, accounting for roughly 12% of the stone-forming population. However, it should be noted that success rates in the elderly are slightly lower than with younger individuals. See below for a summary of a multivariate analysis conducted by Ng and colleagues representing stone-free rate (SFR) in different age groups:
- 40 years old: 54%
- 40-60 years old: 43%
- 60+ years old: 37.6%
Additionally, many studies have suggested that SWL is less effective in elderly patients. The reasoning behind this is not fully understood. However, it is believed that physiological changes in the elderly, such as sclerotic alterations of the renal parenchyma (kidney becomes less flexible as we age) and lower glomerular filtration rate (GFR), contribute to these findings.
TREATMENT OF PAIN
One of the most essential prerequisites for a successful Shockwave Lithotripsy (SWL) procedure is sufficient pain relief for the individual. The entire procedure can be completed with analgesics and sedation only for most. General anesthesia should be reserved for children. Treatment will not be successful if the shockwave energy level decreases due to inadequate pain relief for the individual.
NOTE: During the procedure, you will be connected to oxygen, an ECG, and a blood pressure cuff.
TREATMENT PERFORMANCE
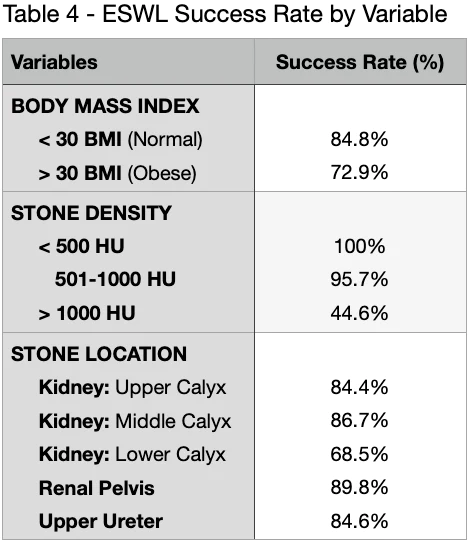
The success rate of Shockwave Lithotripsy (SWL) is dependent on several factors, including:
- Stone density
- Stone size
- Stone shape
- Stone location
- Patient characteristics such as Body Mass Index (BMI).
The average success rate for SWL is between 44-100%. There were no statistically significant impacts related to an individual’s age or sex. However, as mentioned, stone size, density, and location played substantial roles in the success rate of SWL. The following table represents the pooled analysis findings:
POST-TREATMENT FOLLOW-UP
As mentioned previously, Shockwave Lithotripsy (SWL) should be terminated when the destruction of the kidney stone is considered “optimal” or when the further application of shockwaves provides no net gain. When it comes to managing fragments generated from the successful destruction of your stone, several approaches (both natural and pharmacological) are available to you. You will likely be prescribed something out of the Medical Expulsive Therapy (MET) bucket that uses pharmaceuticals if you leave it up to the Doctor. But, Natural Expulsive Therapy (NET) with a product such as CLEANSE is also an option if you want to avoid the litany of adverse side effects associated with MET (click here to learn more about Expulsive Therapy). Either are suitable for assisting with residual fragments from SWL.
If you decide to opt for MET, you will likely be prescribed a type of NSAID to help manage the pain. Unfortunately, NSAIDs are often weak on kidney stone pain and have negative implications on kidney health (learn more here).
NOTE: just because your kidney stone was blasted with SWL, you still have to pass all the residual pieces of the original kidney stone! Which feels the same as passing kidney stones without this procedure. Pain management is critical!
There is also a high likelihood that you will get sent home with a stent to help limit the risk of complications from fragments trying to pass. Unfortunately, stents can be incredibly irritating and sometimes just as painful as the kidney stones themselves.
PRO TIP: Alpha Blocker class drugs have been shown to help with stent irritation. Ask your Doctor to add this to your prescription list if you’ve been sent home with a stent. It’s not a slam-dunk solution. But it’s worth a shot!
Follow-up after your procedure is generally scheduled for 2-3 months out. This provides adequate time for fragments to pass. It is possible to carry out final imaging to verify stone-free status even later in uncomplicated cases. However, earlier follow-up is recommended when it is understood that stone destruction is incomplete and that another SWL procedure will be required. When stones in the kidney have been treated, there is generally no reason to proceed with a follow-up exam until 10-14 days after treatment. The only exception is when symptoms raise suspicion of an obstruction or another type of complication.
CONCLUSION
Exhausting, right? With all the intricacies and tight tolerances, it’s no wonder that this treatment option is on the decline. Plus, it’s expensive at an average cost of $12,000 per procedure with insurance). Since you will also likely require more than one procedure, you are looking at closer to a $24,000 price tag. Our confidence in Shockwave Lithotripsy is pretty low given the inconsistent success rates. We would want to see a 100% success rate for that price tag!
References
- The success of extracorporeal shock-wave lithotripsy based on the stone-attenuation value from non-contrast computed tomography
- How can and should we optimize extracorporeal shockwave lithotripsy?
- A large series of extracorporeal shockwave lithotripsy in the very elderly
- The effect of stone and patient characteristics in predicting extra-corporal shock wave lithotripsy success rate: A cross sectional study
- Extracorporeal shockwave lithotripsy monotherapy for treating patients with bladder stones
- Association between time to lithotripsy and stone-free rate in patients with ureteral stones undergoing shock wave lithotripsy

Written by Joey Weichmann
Joey Weichmann (aka “The Stone Slayer”) is the Founder of Stone Relief. As an avid naturopath and kidney stone sufferer, Joey has made it his mission to help health-conscious individuals stop kidney stones and get their life back.
Comments or questions?
Responses
WHAT TO READ NEXT
Publish Date: December 3, 2023
The Stent Survival Guide
Publish Date: March 28, 2022
American Urological Association (AUA) Guidelines for the Treatment of Kidney Stones
Publish Date: March 20, 2022
Percutaneous Nephrolithotomy (PCNL) for Kidney Stones